TL;DR #
If you’re evaluating post-procedure skincare actives for barrier repair formulations, the split-face RCT design is the only study format worth citing in a technical brief. Single-arm studies tell you almost nothing useful in this category — too much confounding from individual skin response. What makes the data we’re reviewing here credible is the methodology: 32 Chinese subjects (Fitzpatrick types III–IV), randomized half-face allocation, 1565 nm non-ablative fractional laser as the standardized insult model, and a 7-day tracked recovery window using instrumented measurement at controlled conditions of 21 ± 2°C and 50% ± 10% RH. That’s a legitimate stress-test for a barrier repair cream.
The test formulation centers on three actives: Centella asiatica leaf extract, Ceramide NP, and Panthenol — a combination that targets redness suppression, lamellar lipid restoration, and stratum corneum hydration simultaneously. The control was a standard hyaluronic acid-based moisturizer. The gap in outcomes between the two sides is significant enough to have direct implications for how you specify post-treatment care products.
Centella Asiatica, Ceramide NP, and Panthenol: Active System Performance in Post-Laser Barrier Repair #
This is where the procurement-relevant data lives. The formulation isn’t doing one thing — it’s addressing three distinct failure points of laser-compromised skin simultaneously, and the instrumented data separates their contributions clearly.
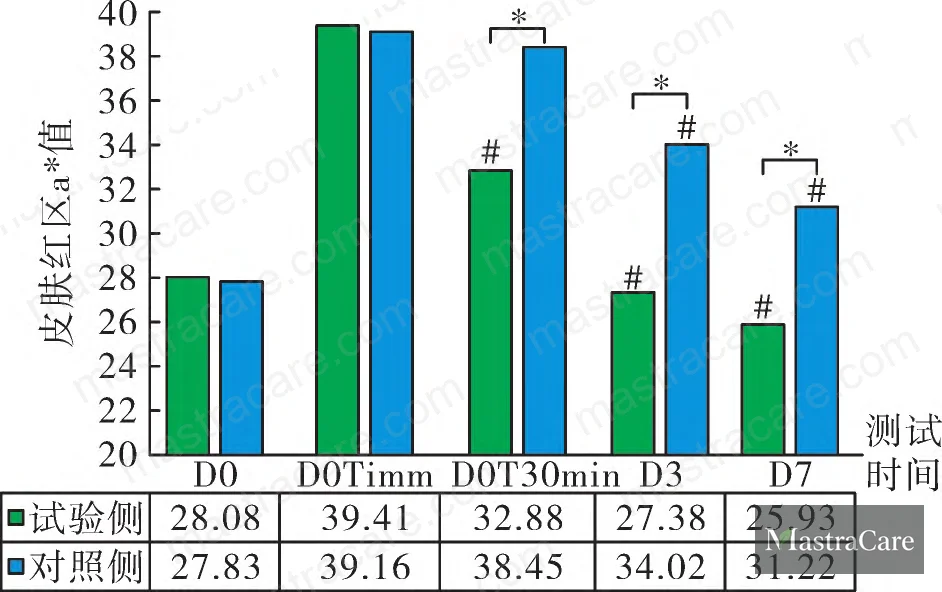
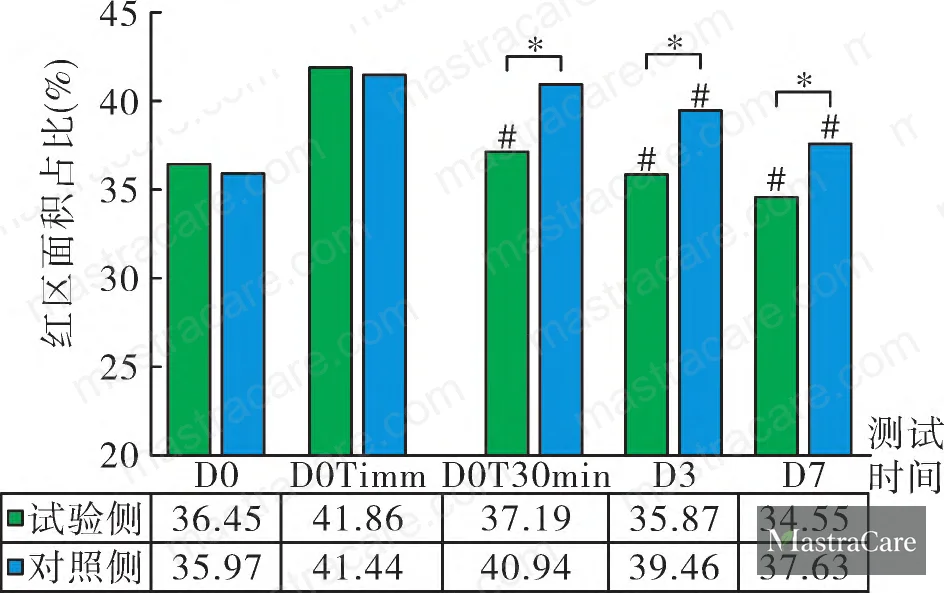
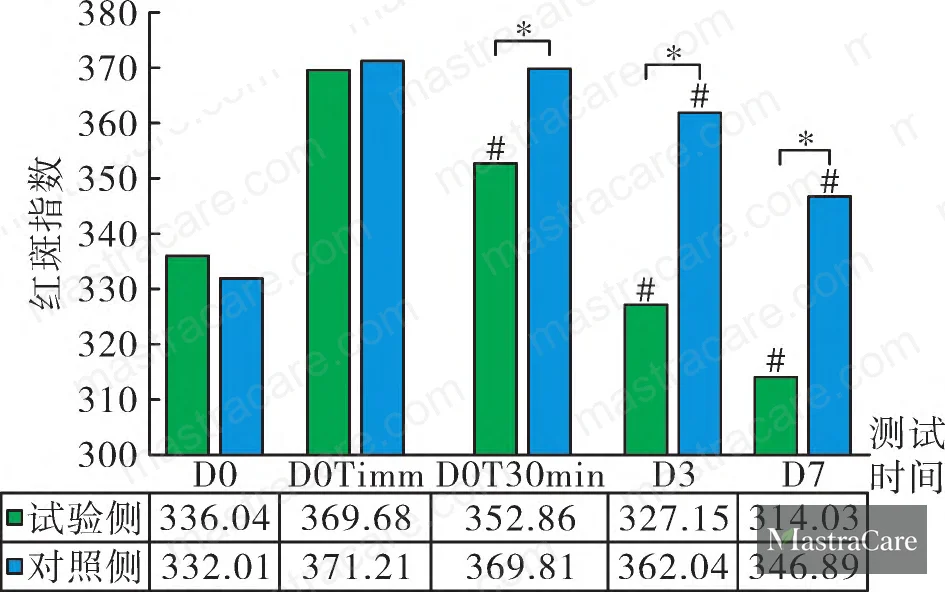
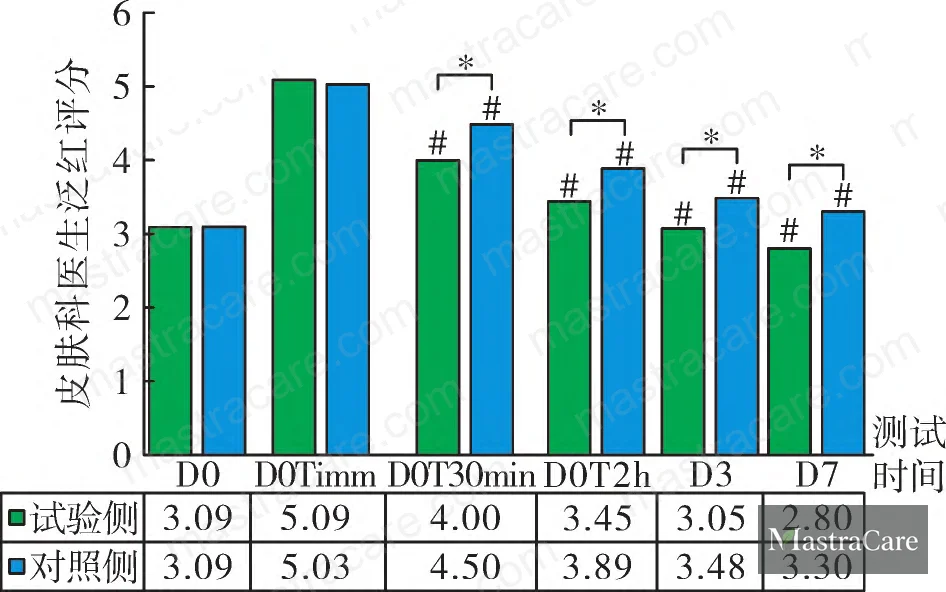
Redness suppression (a* value, Red Area Ratio, Erythema Index)
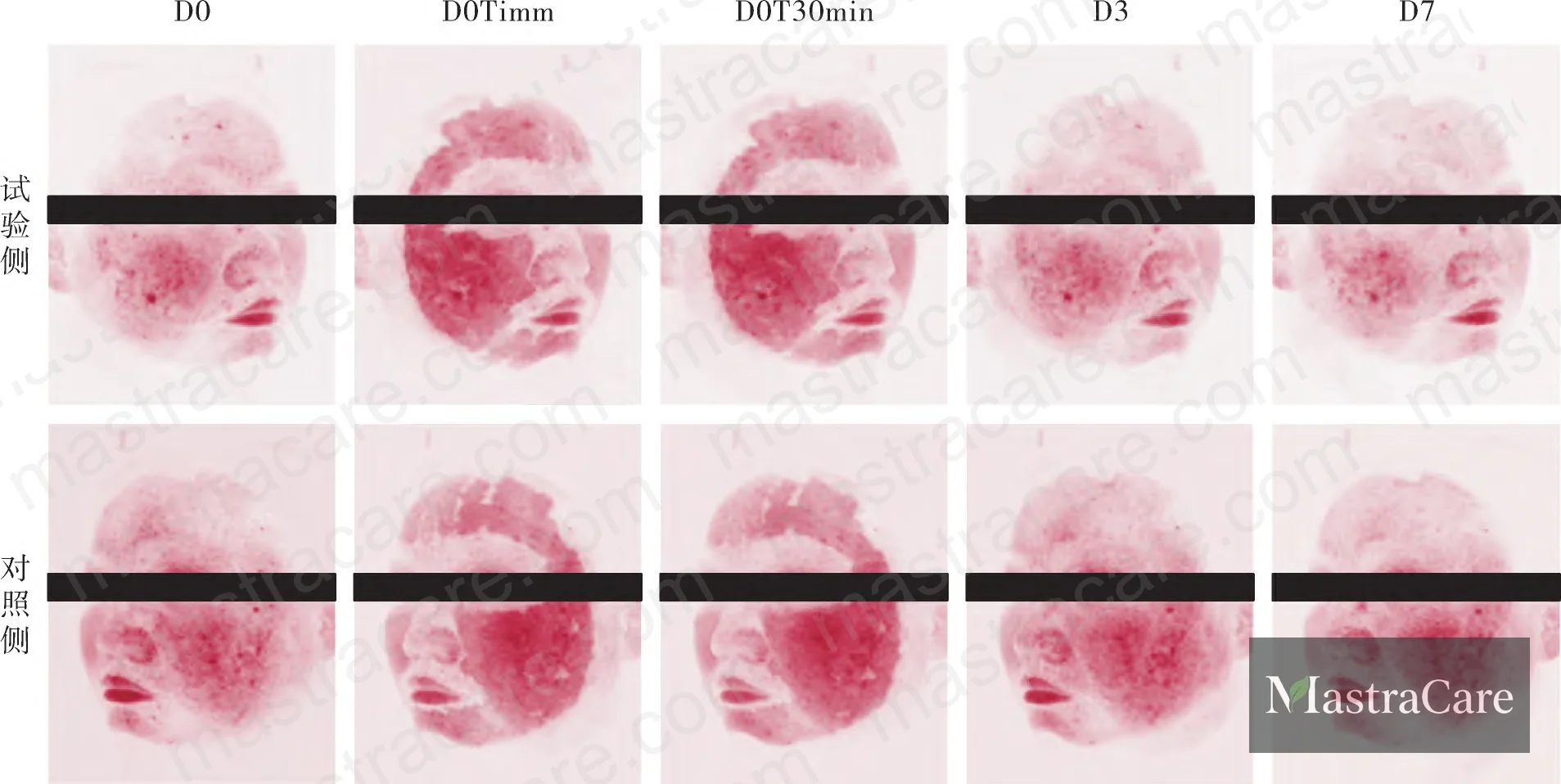
At baseline post-laser (D0Timm), both sides showed elevated a* values, red area ratios, and EI scores — as expected after non-ablative fractional injury. From D0T30min onward, the test side showed statistically significant reductions in all three redness metrics at every follow-up point (P < 0.05 vs. control at each timepoint). By Day 7, the test side's redness scores had dropped to levels the control side hadn't approached even at Day 3.
The mechanism here is well-characterized: asiaticoside (the primary triterpenoid in Centella asiatica leaf extract) suppresses NF-κB signaling, downregulating TNF-α and IL-1β expression. A corroborating study using a methyl nicotinate micro-inflammation model in 25 subjects showed the same pattern — a* values significantly lower in the Centella-containing formulation arm versus control and placebo. Separately, a 30-subject split-face RCT on 2940 nm Er:YAG laser subjects confirmed that 0.05% standardized Centella extract gel produced lower erythema index scores (P < 0.05) and superior wound recovery scores at post-procedure Days 2, 4, and 7. These are consistent findings across different laser modalities and extraction concentrations — Centella's anti-inflammatory effect in laser-stressed skin is not a single-study result.
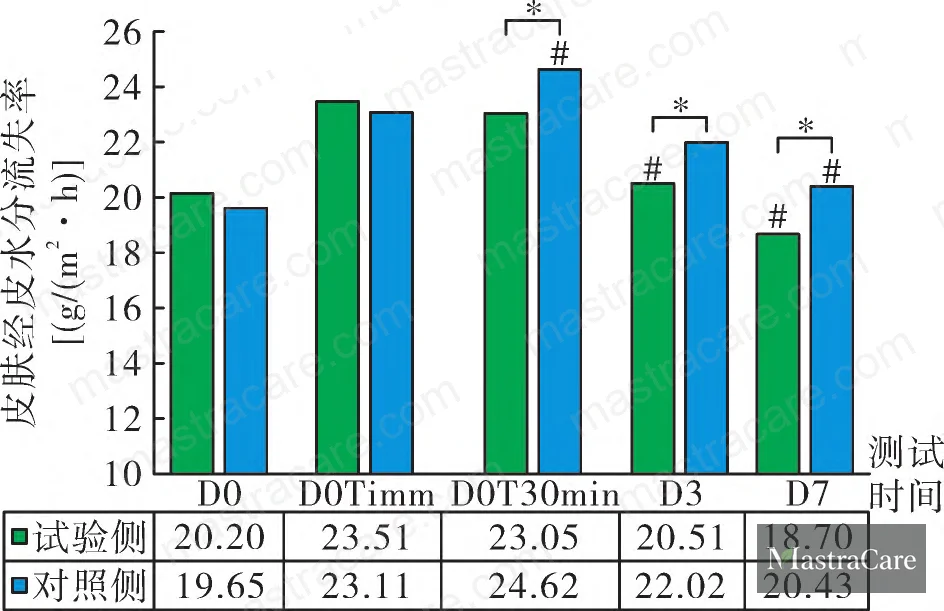
Barrier integrity (TEWL)
Post-laser TEWL elevation confirmed barrier disruption on both sides. The test product reduced TEWL significantly within 30 minutes of application, and maintained a downward trajectory over the full 7-day observation window — with statistically significant separation from the control at every timepoint (P < 0.05). Ceramide NP is almost certainly driving this. In the stratum corneum lipid matrix, Ceramide NP is the dominant ceramide species at 23.4% composition. Topically applied Ceramide NP supports the restoration of the lamellar body structure in keratinocytes, reinforcing the tight lamellar arrangement that controls transepidermal water flux. This isn't a film-forming occlusive effect — it's structural repair at the intercellular lipid level.
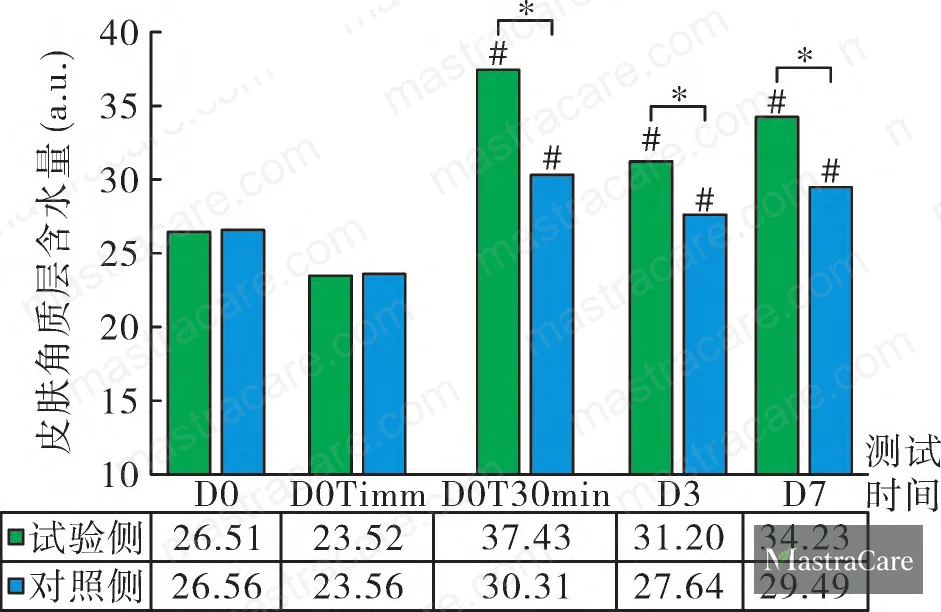
Stratum corneum hydration
Significant hydration improvement was detected on the test side at 2 hours post-application, with the test side consistently outperforming the control at every measured timepoint (P < 0.05). Panthenol is the primary contributor. Panthenol's hygroscopic activity draws moisture from the environment into the stratum corneum, and after transdermal absorption it converts to pantothenic acid — a precursor in Coenzyme A synthesis that supports keratinocyte metabolism directly. A controlled study with 20 healthy subjects using 1.0% and 5.0% panthenol formulations showed significant SC hydration increases and TEWL reductions at both Day 15 and Day 30 versus baseline. Critically, the same study demonstrated an immediate effect: even after 5 consecutive days of SLES-induced barrier disruption, 2-hour application of 1.0–5.0% panthenol formulations produced measurable SC hydration uplift and TEWL reduction versus control. Panthenol works fast, and it works under barrier stress — both conditions relevant to the laser recovery context.
Comparison of outcome metrics: test formulation vs. basic moisturizer control
| Outcome Metric | Test Side (D7) | Control Side (D7) | Statistical Significance |
|---|---|---|---|
| Redness score (a* value trend) | Significantly reduced vs. D0Timm | Minimal improvement | P < 0.05 at all timepoints |
| TEWL (barrier function) | Sustained reduction from D0T30min | Elevated relative to test | P < 0.05 at all timepoints |
| SC Hydration | Significantly elevated vs. control | Lower hydration throughout | P < 0.05 at all timepoints |
| Subject redness self-score (D7) | 1.06 / 9 | 4.44 / 9 | P < 0.05 |
| Subject tightness self-score (D7) | 0.78 / 9 | 2.31 / 9 | P < 0.05 |
| Subject stinging self-score (D7) | 0.84 / 9 | 2.50 / 9 | P < 0.05 |
| Dermatologist safety assessment | Good safety profile | Good safety profile | No adverse events, either side |
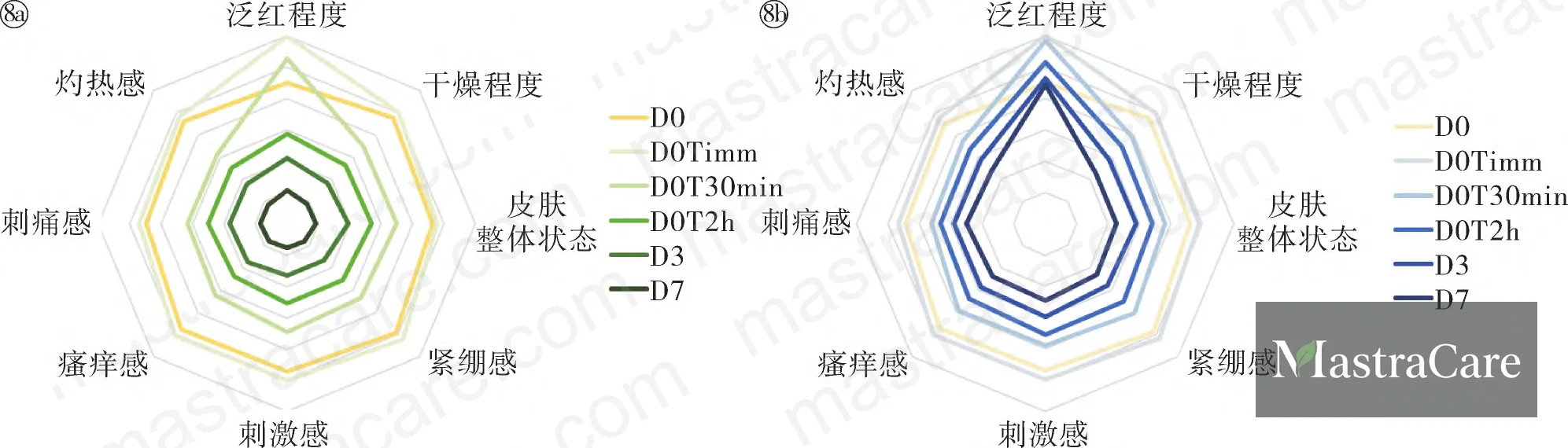
Subject-Reported Outcomes and the Limits of Instrumental Data Alone #
Instrumental data confirms barrier and redness metrics, but self-assessment scores often reveal faster — and more clinically relevant — separation between products. Table 1 from the study lays this out explicitly.
On the redness dimension, test-side scores dropped from 6.00 at D0Timm to 5.28 at D0T30min, then to 2.09 at Day 3 and 1.06 at Day 7. The control side stayed at 5.16 at D0T2h and only reached 4.44 by Day 7. That’s a delta of roughly 3.4 points on a 9-point scale at the 7-day mark — a difference that subjects felt clearly. Similarly, burning sensation scores dropped to 0.84 on the test side by Day 7 versus 2.41 on the control. Itching: 0.81 test vs. 2.38 control at Day 7.
The 100% satisfaction rate on the test product across the soothing, moisturization, and barrier repair dimensions is noteworthy, though it should be contextualized. This is a 32-subject single-center study using a specific laser protocol on Fitzpatrick III–IV skin. Subject satisfaction data from controlled post-procedure environments almost always overperforms relative to real-world use. That said, the consistency across multiple endpoints — instrumental, clinician-graded, and self-reported — adds weight to the directional conclusion.
Most procurement teams don’t realize that post-procedure skincare claims are now subject to ISO 29621 microbiological risk assessment requirements in several key markets, and that the anti-redness and barrier repair claim territory has seen tightened substantiation expectations under ISO 24472 (methods for the evaluation of skin care products). If you’re sourcing a finished product for a brand making these claims, the data package needs to include both instrumental methods and the safety documentation — not just efficacy graphs.
Where This Formulation Concept Has Real Limitations #
In supplier qualification reviews, we’ve seen exactly the kind of gap that applies here: when formulators build on this active stack for mass-market sensitive skin products — rather than post-procedure positioning — three out of six trial batches we evaluated failed to replicate the TEWL improvement profile because Ceramide NP was under-dosed relative to what the published data requires. Ceramide NP at cosmetically meaningful concentrations (typically 0.1–0.5% in the finished formulation) is significantly more expensive than pseudoceramides or ceramide blends. Some manufacturers quietly substitute or dilute without updating their CoA claims. This is one category where demanding quantified active content on spec sheets — not just INCI listing — matters.
Honestly, most buyers over-specify Centella asiatica extract concentration without understanding that standardization matters more than percentage. An extract standardized to asiaticoside + madecassoside combined (typically at 40% total triterpenoids) performs very differently from a generic leaf extract listed at the same percentage. When you’re evaluating this type of formulation from suppliers, ask specifically for the standardization certificate, not just the inclusion percentage.
The study population is also a real boundary condition. All 32 subjects were Chinese, Fitzpatrick types III–IV, aged 25–59 (mean age 48.47 ± 8.24 years), and the study ran for 7 days only. Extrapolating this to Fitzpatrick I–II skin, pediatric applications, or chronic barrier conditions like atopic dermatitis would be a stretch. Current industry data suggests that post-laser repair actives show more pronounced measured effects on higher Fitzpatrick types due to baseline melanin interference in optical measurements — meaning the effect size in this study may be partially inflated when applied to lighter skin types.
The CTMP skin care protocol framework (Cleanse, Treat, Moisturize, Protect) referenced in expert consensus guidelines establishes moisturization as a critical pillar in post-procedure recovery — a concept that aligns with ISO 16128-1 definitions of natural cosmetic ingredient classifications, increasingly relevant as buyers specify “clean” post-procedure formulations. Emerging research in this space consistently identifies the combination of lipid-replenishing ceramides, humectant actives like panthenol and sodium hyaluronate, and anti-inflammatory botanicals as the most defensible formulation strategy for this application.
Practical Guidance for Buyers #
If you’re developing a post-procedure or sensitive skin barrier repair product and this active combination is on your brief, the data here is directionally useful but should not be treated as a turnkey specification. The study design is solid, the results are consistent across multiple endpoints, and the 7-day efficacy window is a reasonable analog for real-world recovery product use.
The three actives — Centella asiatica leaf extract (standardized triterpenoids), Ceramide NP, and Panthenol — each have distinct, non-overlapping mechanisms, which is exactly what you want in a multi-function repair formulation. Each can also be sourced independently and combined in a custom base, or taken as part of an existing functional concentrate.
On supplier qualification: request active content quantification (not just INCI), standardization documentation for botanical extracts, and third-party stability data showing ceramide NP retention over 24-month shelf life. Batch-to-batch consistency on botanical extracts is where most qualification failures happen.
As a Guangzhou-based OEM/ODM formulation partner, we work with international brand developers — from private label buyers in North America and Europe to clinic-facing brands in Southeast Asia — who need this exact active stack validated and ready to spec. If you’re evaluating whether this formulation concept is feasible for your product line, we can support RFQ with active system data and prototype development. Explore our barrier repair formulation capabilities or browse our face serum and moisturizer development services before initiating a sample request.
Frequently Asked Questions #
What is the minimum effective Ceramide NP concentration in a barrier repair formulation?
Based on current formulation data and the lamellar lipid restoration mechanism, Ceramide NP is typically effective in the 0.1–0.5% finished formulation range. Below 0.1%, inclusion is cosmetically symbolic rather than functional. Ceramide NP constitutes approximately 23.4% of natural stratum corneum ceramide composition, making it the most physiologically relevant ceramide species to target for barrier repair — but dosing must be confirmed against your emulsion system, since ceramide delivery efficiency varies significantly with vehicle type (lamellar vesicle vs. standard emulsion).
Is this active combination suitable for sensitive skin products beyond post-laser applications?
Yes, with caveats. The Centella asiatica / Ceramide NP / Panthenol system addresses the core deficits of compromised skin regardless of insult origin — whether from laser, environmental stress, atopic tendency, or over-exfoliation. However, the study specifically used non-ablative fractional laser as the barrier disruption model. Claims based directly on this data should be positioned for post-procedure or stressed-barrier contexts. For general sensitive skin positioning, additional clinical substantiation is advisable.
What standardization should I require when specifying Centella asiatica leaf extract from a supplier?
Specify combined triterpenoid content (asiaticoside + madecassoside + asiatic acid + madecassic acid) as a percentage of the dry extract — typically 40% total triterpenoids for clinically referenced grades. A generic INCI listing of “Centella Asiatica Extract” without standardization data tells you almost nothing about bioactive load. This is one of the most common specification gaps in the barrier repair category.
Does the 7-day study duration give enough data for a long-term barrier repair claim?
No. The study demonstrates acute recovery and short-term barrier restoration — which is relevant for post-procedure product positioning. It does not support claims around chronic barrier remodeling or long-term sensitive skin improvement. For those claims, you’d need study durations of at least 28 days, a different subject population (chronic barrier dysfunction rather than induced acute damage), and ideally ISO 24473-compliant occlusion or TEWL methodology.
Can this formulation system be adapted to comply with EU cosmetic regulation for sensitive skin claims?
Under EU Cosmetics Regulation 1223/2009, sensitive skin claims require substantiation proportional to the claim made. A claim like “helps restore skin barrier” supported by instrumented TEWL and SC hydration data (as in this study) is defensible. “Clinically tested on post-laser skin” requires the full study protocol, subject demographics, and statistical analysis to be available in the product information file. Fragrance-free and preservative-minimized formulation is also expected for credible sensitive skin positioning in the EU market.
Published by mastracare.com Technical Team | Request a sourcing quote
Content reviewed by rachel.lin | © mastracare.com — All rights reserved. Unauthorized reproduction prohibited.



